

Blood Pressure: Why It’s Never Accurate
Blood Pressure: Why It’s Never Accurate
And why it matters.

I have never had my blood pressure taken correctly in a doctor’s office.
Never.
I’ll bet you haven’t either. If you think you have, read on!
But it’s not their fault. They are not given the time, nor the training and incentive to take it properly.
Blood pressure measurement and treatment is the Original Sin of our current Medical System’s failures. We have done this with all “Chronic” Diseases.
It starts with a horribly complex, inconsistent, process to take a measurement that is ripe with opportunities for Human Error. Then prescribes a “treatment” (Pharmaceutical Drug) to treat the symptom, instead of looking for the root cause of the problem so it can be cured/corrected. “Essential Hypertension” is the medical term used most often, which essentially means “cause undetermined”. And the “treatment” inevitably leads to additional symptoms that need treated by, you guessed it: Pharmaceutical Drugs.
Our Modern Medical System is the ultimate Pyramid Scheme.
Let’s take a closer look at this. I’ll start by referring you to this handy-dandy WelchAllyn Quick Reference Guide your doctor’s office SHOULD be using (but probably isn’t). (SOURCE)
Here’s the gist of it, with selected items highlighted and/or comments added by me:
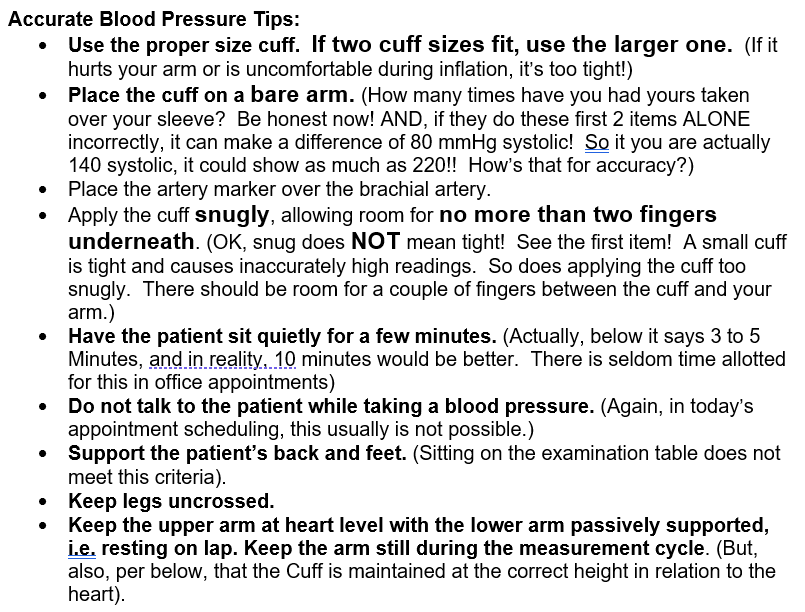
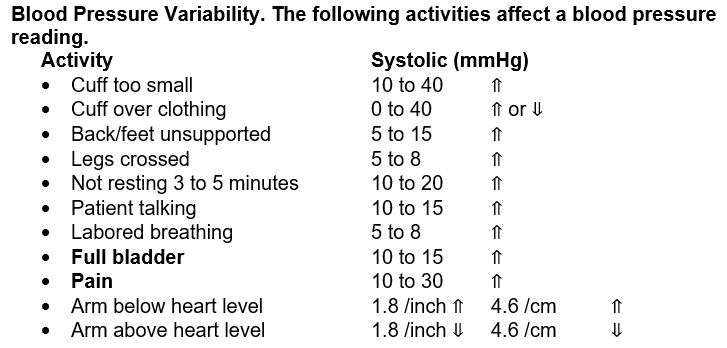
At the end of a clinical appointment, errors made in these measurement activities can increase systolic blood pressure readings by 79.6 to 195.6 mmHg!! OR, decrease systolic readings by14.6 to 44.6 mmHg. Or some combination of the two.
And, ~15% of patients (like me), have “Whitecoat Syndrome”, which means their readings are ALWAYS high in the presence of a doctor or nurse. Throw 80 to 195 Extra mmHg’s on top of that and see what you get!
The net result is that our Medical System is routinely over-medicating patients for HBP. But that’s not all: they are also probably UNDER-Medicating patients that may have LOW blood pressure.
Mind you, I am not suggesting that blood pressure problems don’t exist and don’t need treated (with more emphasis on finding the root cause, and not prescribing a drug). But we desperately need either a method of measurement for blood pressure that is consistent, repeatable, and not as subject to human error as the one we have now, OR we need to do new studies to reset the Blood Pressure standards based on how we currently take blood pressure in the clinical setting. It’s important because our actual measurement practices do not match our diagnostic protocols. The diagnostic protocols were developed based on studies where they DO take the blood pressure meticulously and accurately. We are currently compare apples to oranges.
I first became aware of this in 2007, when I read these studies below commissioned by the AHA that explains all of these issues in even more detail.
Seems like sixteen years should have been long enough for the Medical profession to recognize the problem and find a solution.
But I don’t think anyone is looking. Certainly not the Pharmaceutical Drug Companies who rely on this mess to continue to drive Blood Pressure Medication Sales.
I highly encourage you to read both of these studies listed below. They are written in language that most people can appreciate and understand. I’m not going to break all the disconcerting aspects out for you, because, frankly, there are just too many. I would probably have to write as many pages of explanations about the studies as the studies contain!
But I will give you this one example from my own experience coupled with a quote from the study. Here’s selected quotes from just one section:
“Number of Measurements”
“multiple blood pressure determinations is much greater than a single office reading.”
“first (reading)is typically the highest”
“A minimum of 2 readings should be taken at intervals of at least 1 minute”
“the average of those readings should be used to represent the patient’s blood pressure”
“If there is >5 mm Hg difference between the first and second readings, additional (1 or 2) readings should be obtained, and then the average of these multiple readings is used.”
Now, here’s a one-day section of a chart I made of my own at-home readings in 2007 (yes, the year I originally read these studies):

I took 3 reading, 3 times a day (according to the correct protocol) and plugged them into a spreadsheet to do the math.
You might notice that:
1. During this one day, I had systolic pressure low of 117 and high of 141, and a diastolic pressure low of 74 and high of 87. Some readings fell within the normal range. Some could be considered high.
2. My ongoing average though was fine. It’s the average that matters.
My doctor at the time was trying to convince me to take blood pressure medication, based on 1 office visit (remember I told you I have White Coat Syndrome?). When I declined, he sent me home with a home blood pressure monitor and told me to keep a record of my measurements and come back and see him in 2 weeks. On my return visit he agreed there was no reason for blood pressure medication. And he gave me the monitor to keep!
Here's the studies. It’s worth your time to read them.
Recommendations for Blood Pressure Measurement in Humans and Experimental Animals
Part 1: Blood Pressure Measurement in Humans: A Statement for Professionals From the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research
https://www.ahajournals.org/doi/full/10.1161/01.hyp.0000150859.47929.8e
Part 2: Blood Pressure Measurement in Experimental Animals: A Statement for Professionals From the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research
https://www.ahajournals.org/doi/10.1161/01.hyp.0000150857.39919.cb